Stereotactic Ablative Radiotherapy/Stereotactic Body Radiotherapy (SABR/SBRT). Dr Aznar
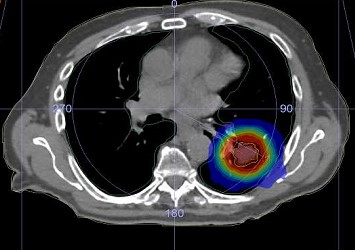
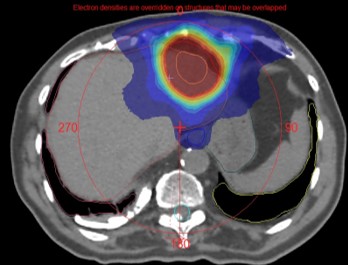
SBRT has been defined by the American College of Radiology (ACR) and the American Society for Radiation Oncology (ASTRO) as the use of very large radiation doses, defined as >6 Gy/fraction delivered in a few (five or fewer) fractions. SBRT has unique radiobiological characteristics that can cause dramatic tumor response, leading to the associated term “ablative” radiation therapy. SBRT requires precise localization of the target volume. “Stereotactic” refers to the fact that SBRT is centered on the target volume and uses online IGRT to localize the tumor in space. The irradiated tissue volume is minimal to reduce toxicity, with a high dose gradient, high conformality, and heterogeneous dose distribution in the PTV. The techniques used can be coplanar or non-coplanar, with IMRT, arc therapy, or cones. The margins are small, dosimetry and dose delivery are complex, and require precise small-field dosimetry.
Below, the techniques and specifics of SABR with a linac are mainly described, and the differences with Cyberknife are also discussed where relevant. SABR with a MRL is described in the slide presentation.
SABR/SBRT is used with high local control and excellent tolerance to treat primary tumours instead of surgery: lung, prostate, pancreas, liver Hepatocellular Carcinomas, Cholangiocarcinomas, Renal cancer…
SABR/SBRT is also very useful in the re-irradiation scenarios.